| Medical Finals contents: Welcome Finals advice Written exams Clinical revision X-Rays Mock final OSCE's |  |
Medical Finals contents: Monthly quiz PDA's Links Credits Your comments Who are we? |
| Medical Finals contents: Welcome Finals advice Written exams Clinical revision X-Rays Mock final OSCE's | |
Medical Finals contents: Monthly quiz PDA's Links Credits Your comments Who are we? |
Question 1 | |||||
This 71 year-old lady suffers from a chronic rheumatological condition.
 Choose the correct combination of hand joints affected and the likely disease that would be in keeping with the above picture. | |||||
| |||||
|
Answer: (e) Rheumatoid arthritis involving the MCP joints and a 'Z'-shaped thumb
Diagnosis of any rheumatologic condition relies heavily on clinical features elicited from the history and examination. The main points to elicit are outlined below:
The differential of an adult onset polyarthritis is outlined in the following box:
The picture above shows a z shaped thumb and subluxation with ulnar deviation of the MCP joints. Hand signs are legion in rheumatological disease and some of the main abnormalities are outlined in the box below:
In summary, examination of the hand is a popular examination OSCE that can be used in basic clinical skill exams through 3rd MB to Final MB. Rheumatoid arthritis is present in around 1% of the population and is more frequent in women than men. It affects the hand in the majority of patients and deformity is an easy clinical observation. Most importantly, the diagnostic criteria for RA are largely clinical and the condition is one that carries a high degree of morbidity and mortality. It is always important to consider this condition and be aware of the pharmacological interventions and appropriate referral of patients who may have it. |
Question 2 | ||||||||||||||||
A 65 year-old arteriopath had a carotid endarterectomy in the past 2 weeks following recurrent episodes of amarosis fugax.
 | ||||||||||||||||
| ||||||||||||||||
|
Answer: (d) 70%
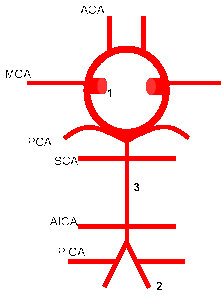
Stroke is one of the most common causes of mortality and morbidity in the western world and this patient has presented with symptoms suggesting a transient ischaemic attack, a major warning that a stroke is likely to occur in the immediate future. TIA is a heterogeneous disorder and presenting syndromes depend both on the extent of vascular pathology and territory of blood vessels involved. Understanding the heterogeneous syndromes that can present requires knowledge of the blood supply to the brain and the functions of each vascular territory with respect to cerebral function. Figure 2 outlines the circle of Willis and its main branches. The anterior circulation, from the internal carotid artery (ICA), consists of the middle and anterior cerebral artery which supply the lateral and medial surface of the cerebral cortex and deeper structures of the cerebral hemisphere such as the basal ganglia. The ICA also gives off the ophthalmic artery, hence the episodes of amarosis fugax that can occur. The posterior circulation arises from the vertebral arteries and the basilar artery. These vessels give off branches that supply the occipital cortex, brain stem and cerebellum:
Anterior circulation strokes typically present with hemisensory / motor symptoms affecting the face and limbs with monocular visual impairment, whereas posterior circulation strokes present with bilateral motor or sensory symptoms and bilateral visual impairment. When the cause of TIA is attributed to a stenosis of the internal carotid artery, it is possible to perform a carotid endarterectomy (CEA) to relieve the symptoms and prevent future occurrence of a stroke. However, this procedure is associated with a significant risk of stroke and death that varies depending on the patient's presentation. This can be grossly divided in to asymptomatic and symptomatic, with further division of symptoms depending on the nature of the event as is shown in table one below. Table 1 adapted from: Bond R, Rerkasem K, & Rothwell PM, (2003) "Systematic review of the risks of carotid endarterectomy in relation to the clinical indication for and timing of surgery", Stroke, 34(9), 2290-2301.
In general, the benefit of CEA versus the risk of post operative stroke is considered to be favorable when there is a 70% stenosis in symptomatic patients. However, as studies are published, the heterogeneity of TIAs is being realized as an important factor in the determination of post-operative outcome as is shown above. Other interventions, such as carotid stenting, have been shown to have excellent results in specialist centres. | ||||||||||||||||
Question 3 | ||||||
This 64 year-old man has been suffering from osteoarthritis in both knees for several years.
 Which joint in the hand is he most likely to have similar problems with? | ||||||
| ||||||
|
Answer: (c) 1st carpometacarpal joint
Just like in rheumatoid arthritis, the clinical features of osteoarthritis are key in determining the diagnosis. In the hand, OA involvement of the 1st carpometacarpal joint leads to squaring of the thumb, involvement of the DIP joint leads to Heberden's nodes and involvement of the PIP joints to Bouchard's nodes. Investigation of OA is by x-ray of the involved joints, which can also be used to grade severity and monitor progression of the disease. It is important to be able to distinguish the features of rheumatoid arthritis and OA and these are outlined in the box below:
Squaring of the thumb is not to be confused with the RA deformity of a Z-shaped thumb. Squaring is best seen by looking at the base of the thumb at the wrist on the dorsal aspect of the hand. Management of OA and any other musculoskeletal disorder that affects ability to perform activities of daily living is multidisciplinary and aimed at maintaining function and relieving pain. Therefore, physiotherapists and occupational therapists have a significant role to play in the management of these disorders. Pharmacological relief of pain utilizes simple analgesics such as paracetamol and non-steroidal anti-inflammatory drugs. Codeine is a useful adjunctive analgesic. Intra-articular corticosteroids and hyaluronic acid may also be used. Surgical treatment, especially joint prostheses, play a major role, especially with large joints like the hip and knee. | ||||||
Question 4 | |||||
|
An 84 year-old nursing home resident is admitted with vomiting and a grossly distended abdomen. AXR is highly suggestive of a sigmoid volvulus.
Which other patient group is susceptible to sigmoid volvulus? | |||||
| |||||
|
Answer: (e) Psychiatric patients
A sigmoid volvulus is defined as a twisting of the sigmoid colon resulting in obstruction and impairment of the blood supply. There are three types of gastrointestinal tract volvulus:
Sigmoid volvulus is associated with:
Presentation is with bowel obstruction with a distended abdomen and vomiting. Causes of Bowel obstruction:
Diagnosis is by abdominal x-ray, water soluble single contrast enema or CT abdomen in which the coffee bean sign, bird of prey and whirl sign are useful features that point to a sigmoid volvulus. The treatment of choice for a sigmoid volvulus is decompression with a rectal tube, however recurrence is common. |
Question 5 | ||||||||||||||||||
|
A 56 year old male patient is admitted to your surgical ward on take with a history of abdominal pain, diarrhoea, malaise and fever.
His past medical history reveals that he was treated conservatively for diverticulits three weeks ago and has been feeling unwell for a few days. On examination, his abdomen is soft with mild tenderness and guarding in the left iliac fossa. There is a palpable mass on rectal examination. His temperature is 37.7°C but otherwise stable. What condition would you think of first when ordering a CT Abdomen? | ||||||||||||||||||
| ||||||||||||||||||
|
Answer: (b) Pelvic abcess
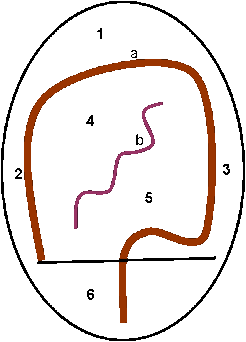
With any patient of this age it is always prudent to be concerned about potential neoplastic disease. However, a history of recent gastrointestinal inflammation or surgery would raise the index of suspicion for an intra-abdominal abscess. Clinical features are relatively vague, mild and also vary according to the intra-abdominal compartment involved. A pelvic abscess can present with diarrhoea, tenesmus, urinary frequency or mucus in the stool and can result in a fluctuant mass being palpated on rectal or vaginal examination. This emphasizes the clinical importance of performing a rectal examination, at least in patients presenting with an acute or subacute abdomen. As was the case with this patient, localized sepsis associated with diverticulitis, a disease that is limited to the distal colon, can result in pus formation which can drain down into the pelvis to form an abscess. Investigation is by ultrasound and CT scan. Treatment is by drainage which can be percutaneously guided by radiological methods.
There are various compartments in the abdomen that act as natural sumps for pus from localized sepsis to collect in. They are dependant areas of the abdominal and pelvic cavity formed by solid organs and overlying peritoneum.
|