| Medical Finals contents: Welcome Finals advice Written exams Clinical revision X-Rays Mock final OSCE's |  |
Medical Finals contents: Monthly quiz PDA's Links Credits Your comments Who are we? |
| Medical Finals contents: Welcome Finals advice Written exams Clinical revision X-Rays Mock final OSCE's | |
Medical Finals contents: Monthly quiz PDA's Links Credits Your comments Who are we? |
|
A 43 year-old carpet fitter presented to A & E with an acutely swollen tender red, hot right knee. On examination he is unable to fully extend the right knee. The patellar tap test is positive.
Aspiration of his right knee was performed. The aspirate is shown.  What is the most likely diagnosis? |
| (a) Gout |
| (b) Bursitis |
| (c) Pseudogout |
| (d) Septic arthritis - THE CORRECT ANSWER |
| (e) Ruptured Baker's cyst |
|
(d) Septic Arthritis
A patient with an acutely swollen tender, red, hot joint should be assumed to have septic arthritis until proven otherwise. Untreated septic arthritis can destroy a joint within days. The definitive diagnosis is made by joint aspiration. The appearance of the aspirate may be helpful, but ultimately microbiological analysis for organisms, culture and sensitivity is required. Intravenous antibiotics (Flucloxacillin and Fusdic acid) must be commenced with immediate effect. The commonest causative organism is Staphylococcus aureus. Antibiotic treatment must be for at least 6 weeks, with a minimum of 2 weeks of intravenous antibiotics. The aspirate shown is turbid suggesting septic arthritis as the likely diagnosis. The diagnosis of gout/pseudogout is made by identification of the presence of crystals within a joint aspirate. Gout: Negatively befringent crystals Pseudogout: Positively befringent crystals Occupations requiring time resting on the knees, such as carpet fitters, are prone to bursitis, but also septic arthritis as breach of the skin may form a portal of entry. |
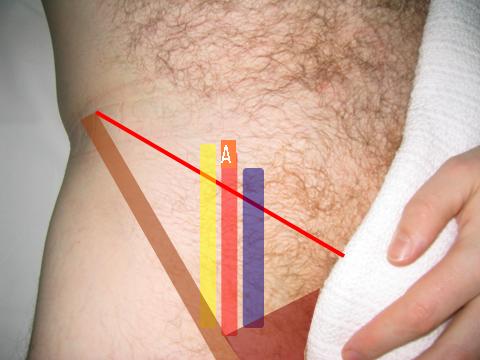 Which of the following structures is labeled A on the photograph? |
| (a) Femoral artery - THE CORRECT ANSWER |
| (b) Femoral Vein |
| (c) Femoral Nerve |
| (d) Inguinal Ligament |
| (e) External Iliac Vein |
|
(a) Femoral artery
The femoral triangle is an important anatomical area. Contained within are the femoral artery, femoral nerve and femoral vein. From medial to lateral:
The boundaries of are:
Identification of the femoral artery is important clinically. It is located at the mid-inguinal point (mid way between the anterior superior iliac spine (ASIS) and the symphysis pubis in the midline. It may be identified for:
The external iliac artery becomes the common femoral artery as it passes under the inguinal ligament. Anatomy of Arteries (branches):
|
A 27 year-old mechanical engineer attended his GP over concerns regarding an intermittent erythmatous rash. It is not noted to be related to any specific exposure. He is allergic to aspirin. The rash is shown below.
 What is the correct term for the appearance seen in this picture? |
| (a) Koebner's phenonmenon |
| (b) Dermographism - THE CORRECT ANSWER |
| (c) Urticaria |
| (d) Pityriasis rosea |
| (e) Guttae psoriasis |
|
(b) Dermographism
The appearance is classical of dermographism. The skin reacts in a weal type manner to pressure - thereby enabling a patient to write words on the skin. It may be a feature of urticaria, although can occur in a normal individuals. Urticaria is a transient, itchy, erythematous histamine-led reaction of the skin which is frequently recurrent in nature. It may be related to a definite causative agent, such as shell-fish, but commonly is idiopathic. Treatment is with oral antihistamine medications. A small number of patients will also suffer from angioedema or anaphlactoid reactions require the need to carry an epi-pen (IM adrenaline) at all times. |
| Which of the following pieces of information is the most helpful in obtaining or in rejecting a diagnosis of epilepsy? |
| (a) EEG result |
| (b) MRI scan result |
| (c) Enhanced CT scan result |
| (d) Accurate history and eye-witness account - THE CORRECT ANSWER |
| (e) Patient reports tongue biting and incontinence |
|
(d) Accurate history and eye-witness account
Always remember that epilepsy is essentially a clinical diagnosis and relies heavily on an accurate history and on a reliable eye-witnessed account. All the other investigations come secondary and are supportive rather than diagnostic. In 30% of patients with epilepsy their EEG is normal. Even in the normal population who do not have epilepsy there can be abnormalities if an EEG is performed. Therefore an EEG is supportive and can be helpful in the treatment and planning surgical options, but is not a diagnostic test. Neuroradiology (CT and MRI) can help in isolating a focus for localisation related epilepsy, but again the diagnosis of epilepsy lies in the clinical history. |
| Which of the following is more likely to represent a patient suffering from an epileptic seizure as opposed to a syncopal event? |
| (a) Presence of some limb jerking |
| (b) Regaining consciousness in an ambulance - THE CORRECT ANSWER |
| (c) Regaining consciousness in the immediate surroundings |
| (d) An un-witnessed event |
| (e) Eye-witness reports skin pallor |
|
(b) Regaining consciousness in an ambulance
It is important to be able to distinguish syncope from epilepsy and also from non-epileptic attack disorders. Syncopal episodes are almost always situational, occurring in the context of standing, hot environments, in school assembly, in queues and in pubs. There are usually reports of pallor, sweating, tinnitus and tunnel vision. The episode is short lived, and individuals more often than not regain consciousness in the situation where they originally lost it! Anoxic jerks are not uncommon if the syncopal event occurs in the up-right posture. This occurs in response to the lack of oxygen and blood supply to the brain it responds with a few anoxic jerks. In epileptic seizures awakening in the ambulance signifies a much more prolonged loss of consciousness and therefore is more associated with epilepsy than a syncopal event. Here is a table comparing epilepsy with syncope: Comparative features of syncope and seizures:
|
Thanks to everyone completing the quiz last month (February 2006) from Riyhad to Hong Kong, Dublin and more.