Please find below a number of new radiographs for your interest. At medicalfinals.co.uk we aim to continue to add new locally sourced clinical material to help pass finals. Any suggestions would be welcomed and in future the team hope to introduce material to assit with written as well as clinical finals.
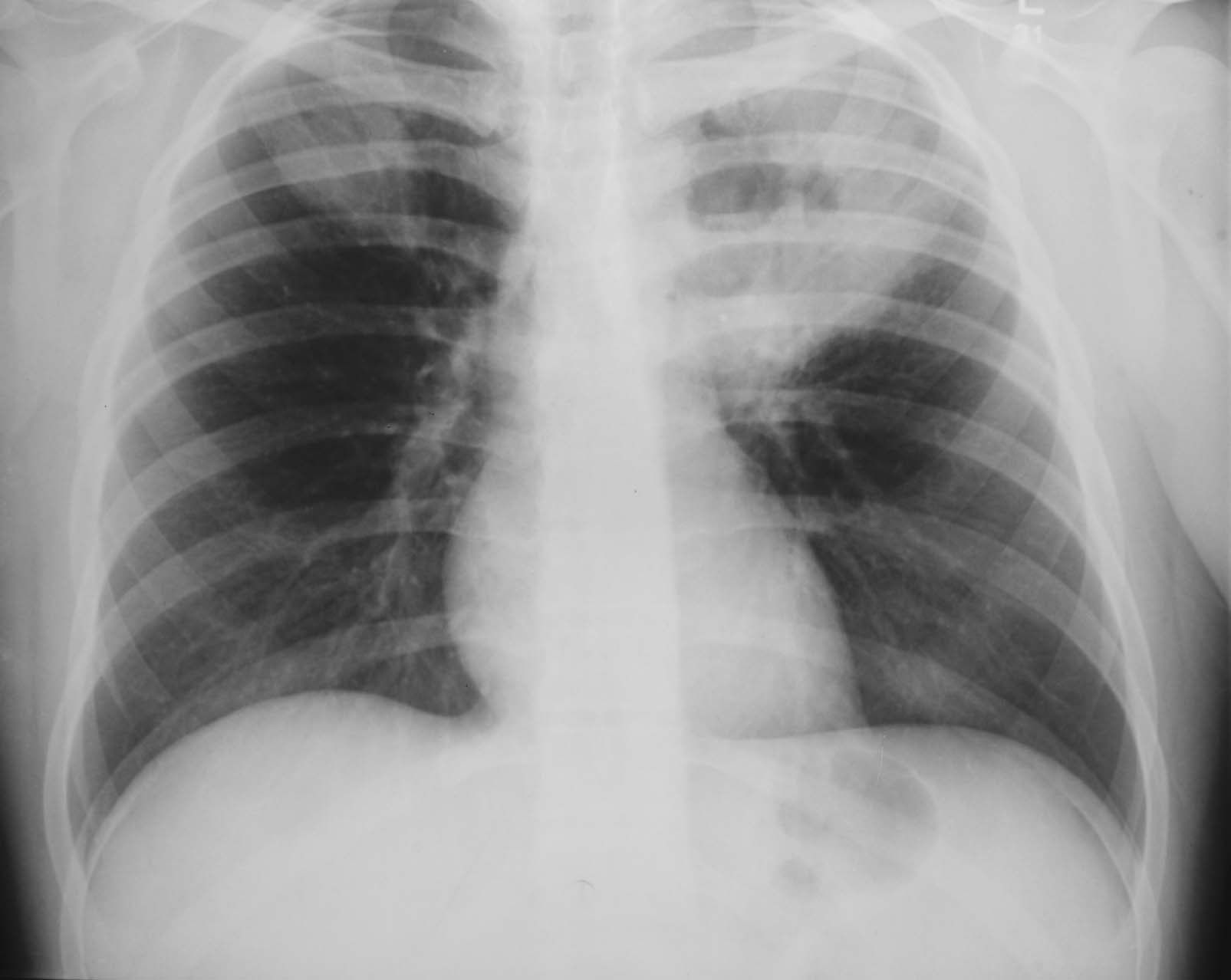
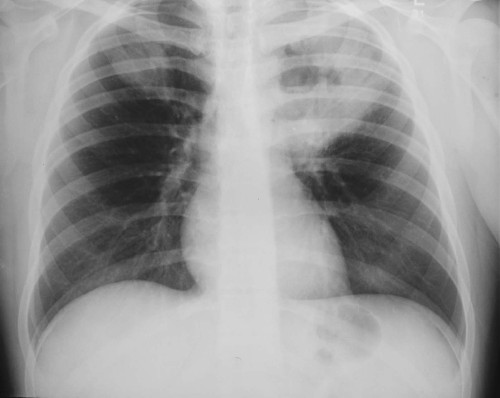
Mitral Stenosis (figure 1):

|
Features:
- Double right heart border (right atrium/ventricle and enlarged left atrium)
- Splaying of the subcarinal angle (seen here as 90 degrees. Usually less than 60 degrees)
- Cardiomegaly (cardiac failure has followed the long standing valve disease)
|
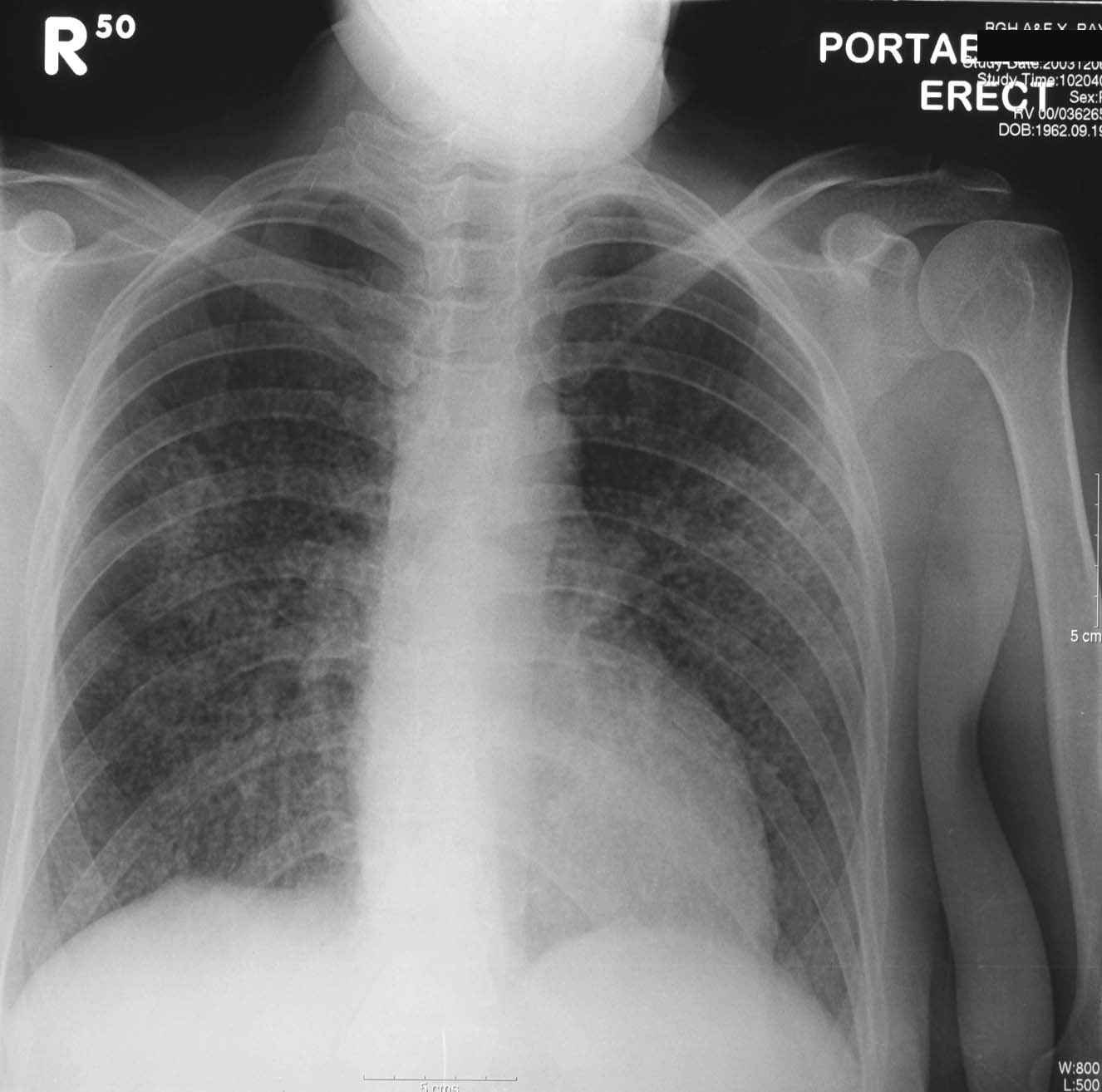
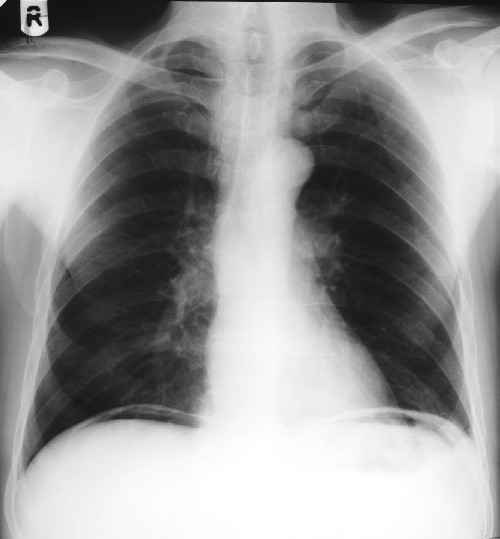
2. Retrosternal Thyroid (figure 2):

|
Features:
- An enlarged superior mediastinum is noted extending to the neck.
- An area of calcification can be seen within, likely a thyroid nodule of some duration.
Note: superior mediastinal masses can be further subdivided into anterior, middle or posterior mediastinum. A retrosternal thyroid is a superior anterior mediastinal mass.
|
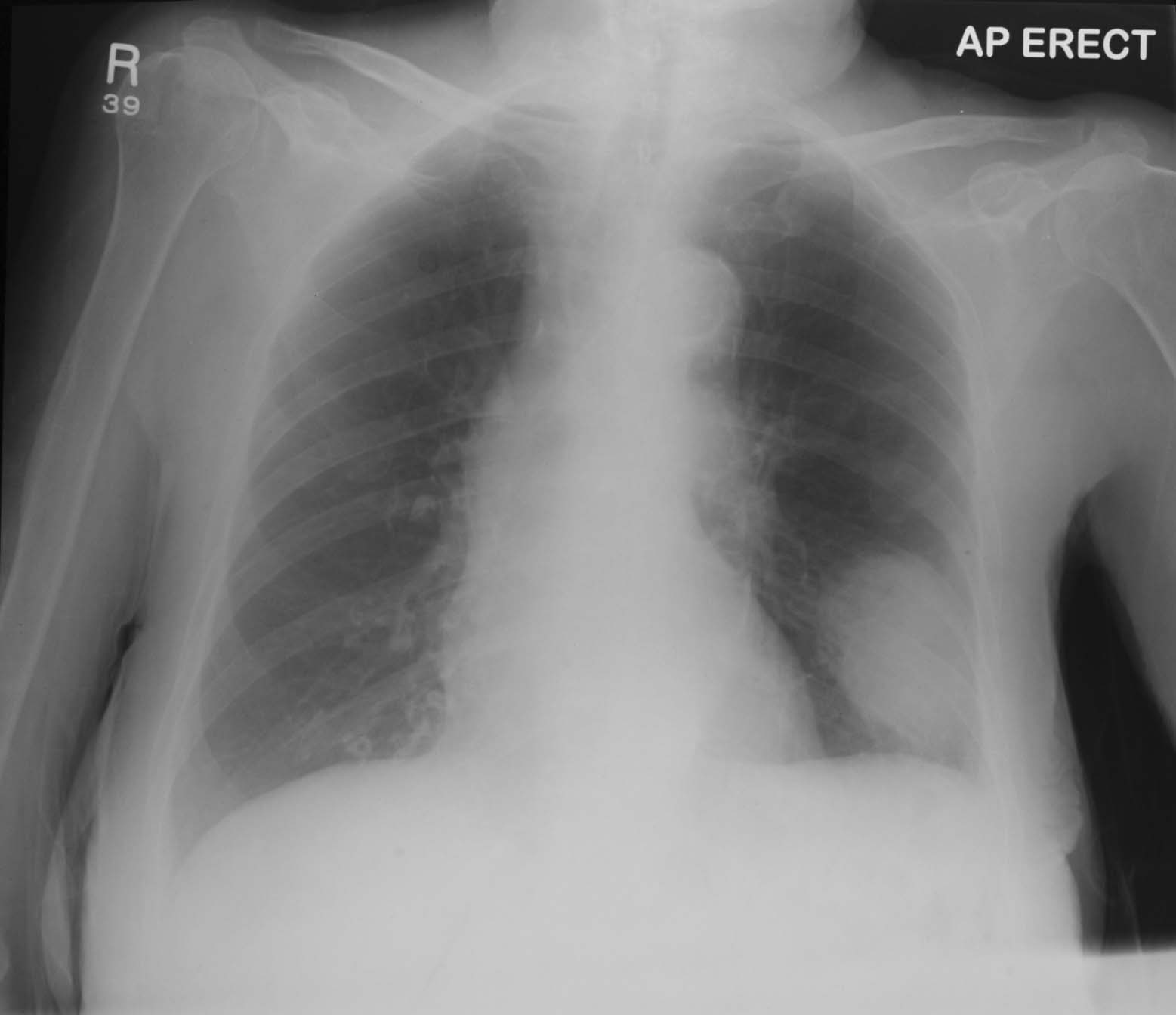
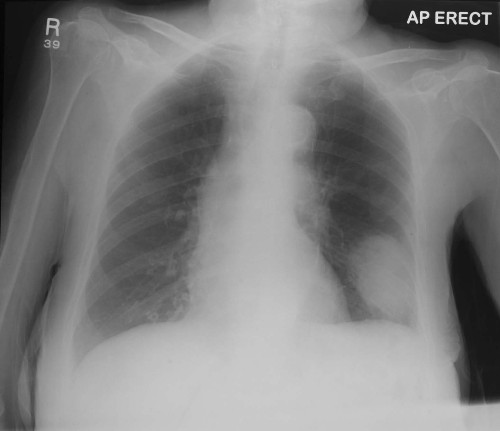
Left Upper Lobe Consolidation (figure 3):
|
Features:
- Consolidation of the left upper lobe (cavitating in nature).
- Loss of the silouette of the aortic knuckle
- Smaller area of consolidation in contralateral right upper lobe
Note: Final diagnosis was Wegner's granulomatosis. This is a classical cause of a cavitating chest lesion. Others include squamous cell bronchial carcinoma and tuberculosis.
|
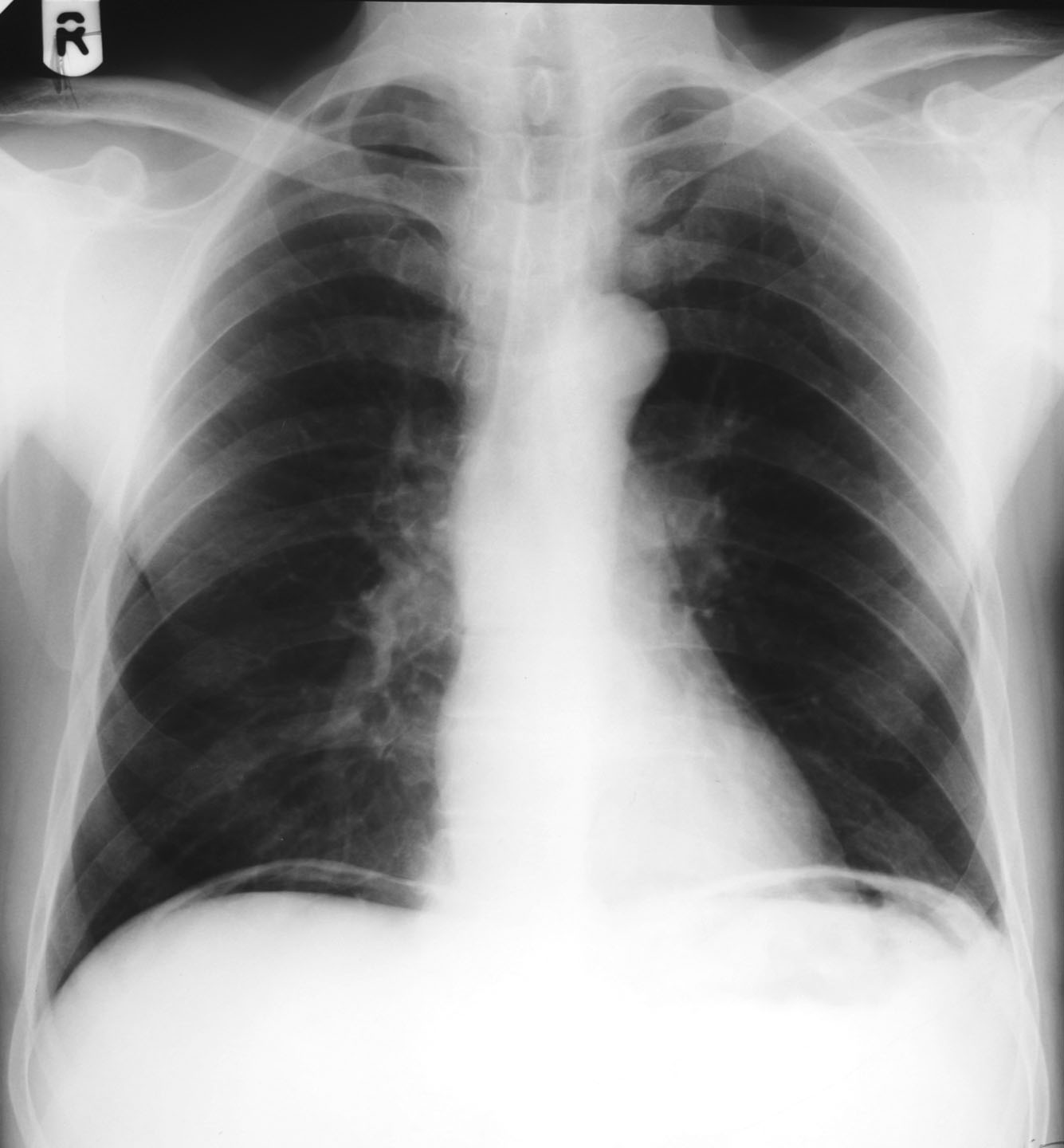
Cystic Bronchiectasis (figure 4):

|
Features:
- multiple cystic areas in the right lower lobe
Note: In the under 20 year-old always consider cystic fibrosis 1st if cystic changes are seen on CXR.
|
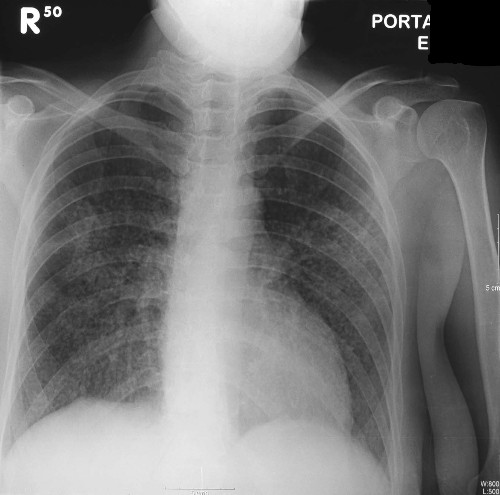
Miliary Shadowing (a unusual film with mostly uncommon causes) (figure 5):
|
Features:
- multiple 1-2mm nodulars throughout all lobes of both lung fields
Differential Diagnoses: Miliary tuberculosis, metastases from papillary carcinoma of the thyroid, varicella pneumonia, histoplasmosis.
|
Large Broncial Carcinoma (figure 6):
|
Features:
- Large left lower lobe bronchial carcinoma
|
Pleural Effusion (figure 7):

|
Features:
- Moderatly sized left sided unilateral pleural effusion
Note: Unilateral pleural effusions are typically exudative and bilateral transudates.
|
Ventricular Aneurysm (figure 8):

|
What is most likely cause of this x-ray findings?
It is most likely that this individual had a past myocardial infarction leaving a area of 'dead' unfunctional myocardium.
This non-contractual myocardium in the long term can develop into an aneurysm.
|
Pneumothorax (figure 9):

|
What underlying conditions predispose to pneumothorax?
Young, tall asthenic men (pulmonary blebs) and those with lung disease such as cystic fibrosis, emphysema, asthma, Marfan's, HIV.
|
Pneumoperitoneum (figure 10):
|
What are the causes of a pneumoperitoneum and the radiological signs if the film is taken supine?
- Peptic ulcer perforation
- diverticular perforation
- bowel perforation following obstruction
- post laproscopic surgery (CO2 used for insufflation)
Rigler's sign (gas seen on both sides of the bowel wall) and Falciform Ligament sign (falciform ligament seen due to gas on both sides of it within the peritonem) are two described signs of a pneumoperitoneum on supine plain AXR.
|