These are good X-ray images to review, along with self-test questions and answers. Further images will be added over time.
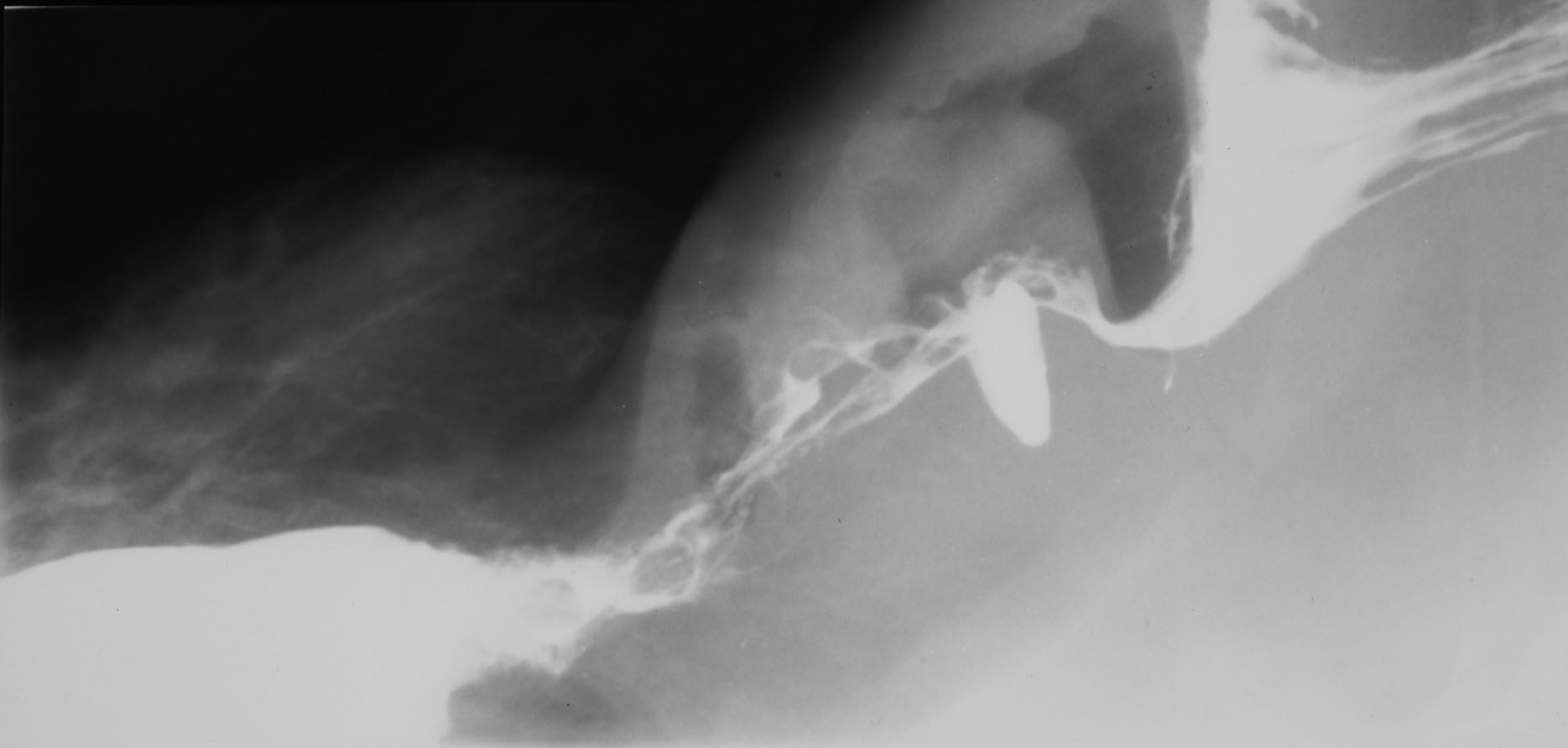
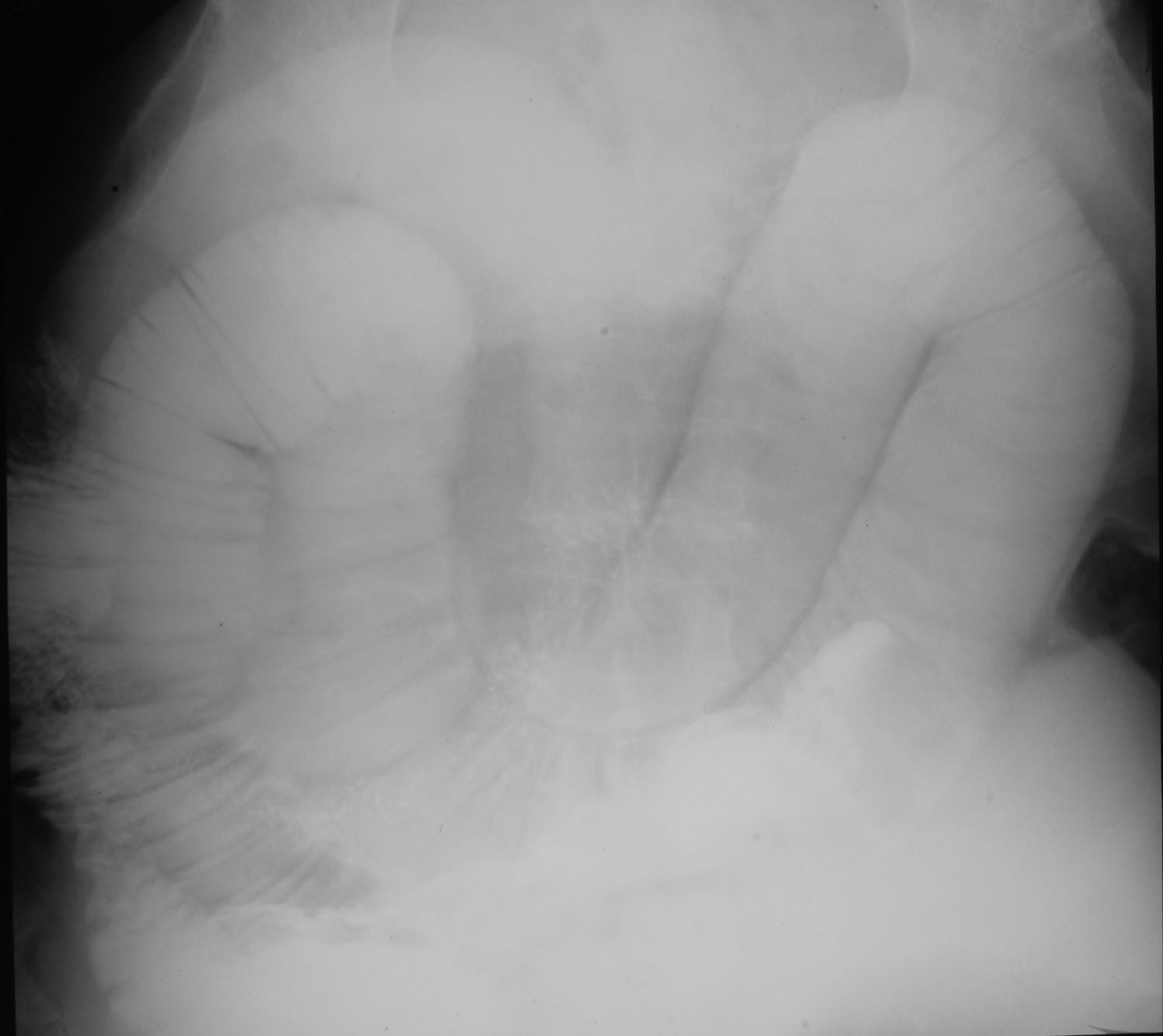
Oesophageal Carcinoma (figure 1):

|
Explain the reason for the huge increase in oesophageal adenocarcinoma?
Oseophageal adenocarcinoma is the most rapidly increasing malignancy in the western world. It is believed to be due to the high prevalence of gastro-oesophageal reflux disease (GORD) reflective of the western lifestyle. This in itself can cause Barett's oesophagitis which is a precursor to adenocarcinoma in a proportion of individuals. The metaplastic epithelium of the lower oesophagus secondary to reflux can progress from dysplasia through to adenocarcinoma, hence a biannual OGD for screening purposes.
|
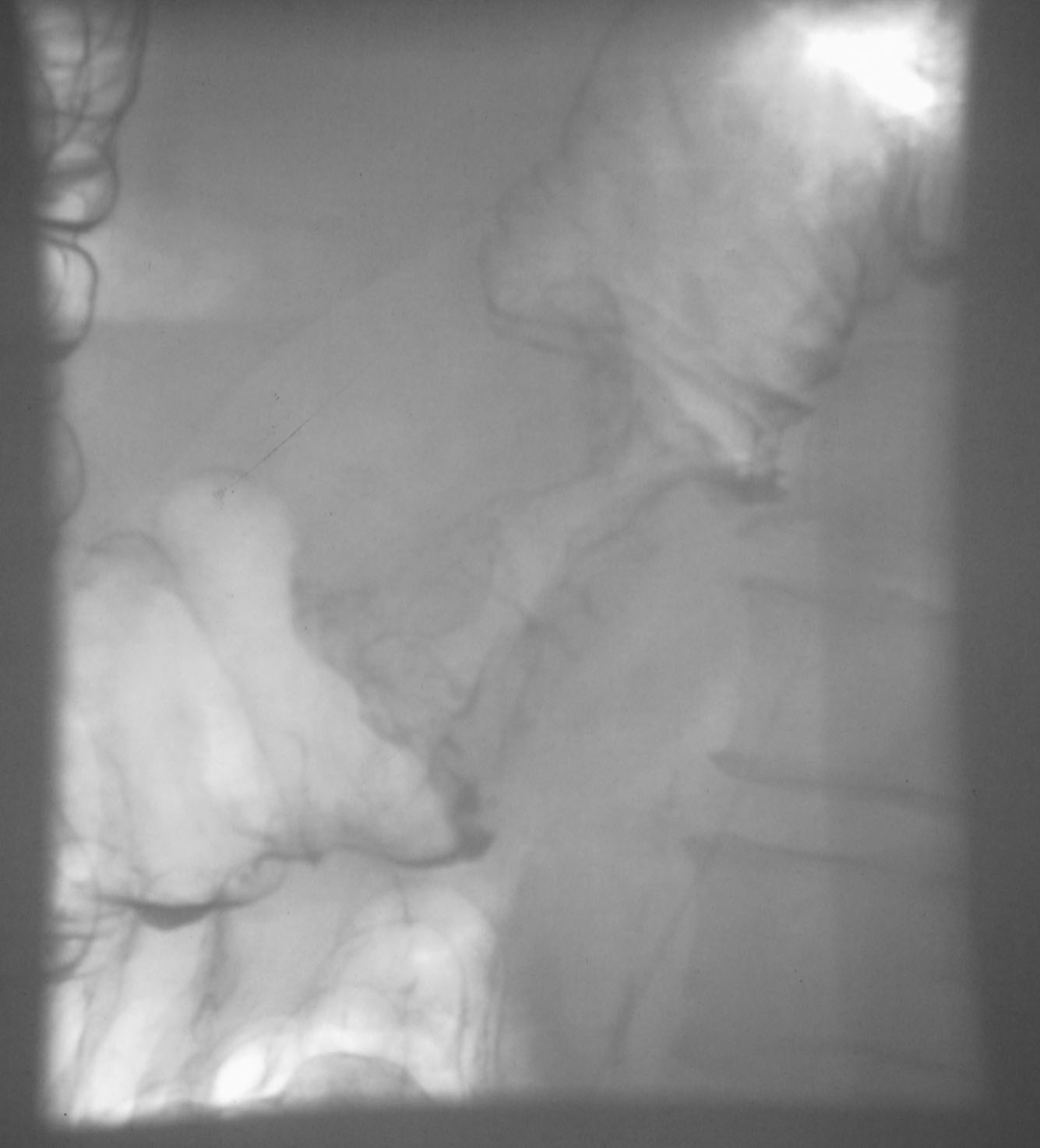
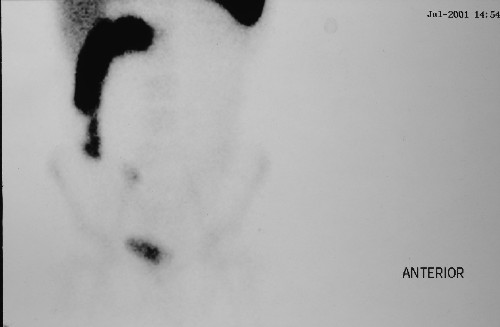
Ulcerative colitis (figure 2):
|
Explain the purpose and findings of this scan.
This is a radio-labeled white cell (SEROTEC) scan. This is a
nuclear imaging procedure whereby 100mls of venous blood are labeled
with a radio-isotope (technetium 99m) and re-injected and then
followed by gamma camera. The white cells are attracted to areas of
inflammation. It helps to explore the extent and distribution of
inflammation in inflammatory bowel disease. In this case there is
increased uptake in the proximal ascending colon and rectum.
|
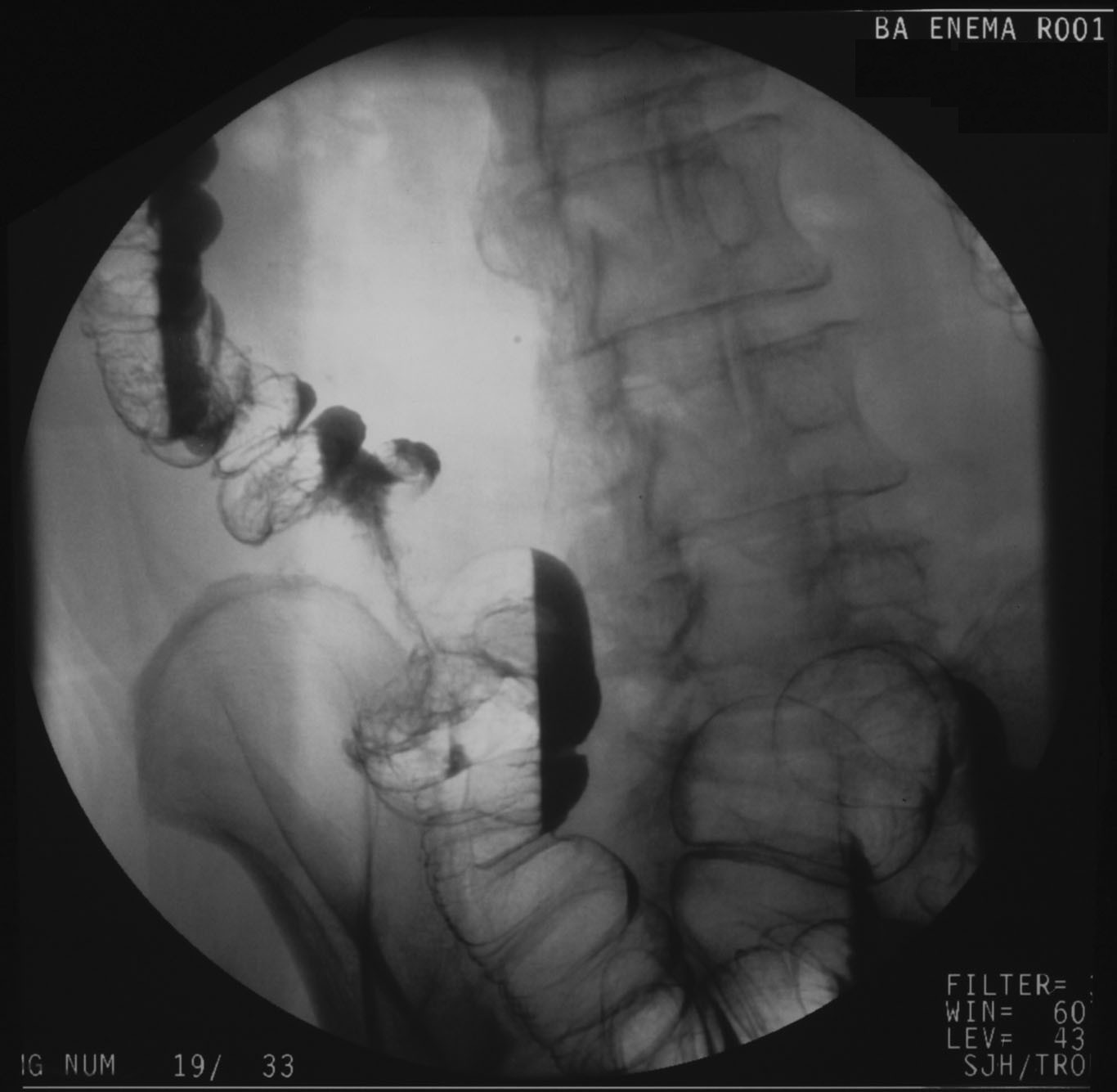
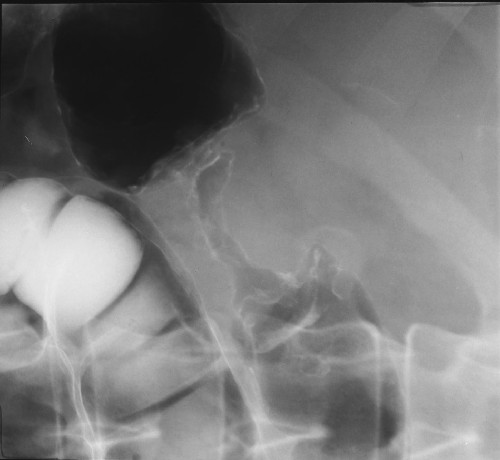
Colorectal Carcinoma (figures 3,10,11,13):


|
Describe the features of these images and how these tumours are classified?
These three double contrast barium enemas illustrate fine examples
of apple core strictures from annular colorectal carcinomas.
The position of the tumour within the large bowel dictates the
operative procedure and the histological diagnosis will influence
whether adjunctive chemo/radiotherapy is used.
Duke's classification is widely used - the original
described A,B, and C with the latter addition of D.
- A: confined to mucosa
- B: Extended through all muscle layers to serosa
- C: as for B and lymph node metastases
- D: distant metastases.
|
Gallstones (figure 6):

|
What percentage of gallstones are seen on AXR? Are gallstones significant in themselves?
10-15% of gallstones are seen on plain AXR and their presence in themselves do not indicate they are causing an acute illness. Gallstones often remain in the gallbladder for years without any trouble.
|
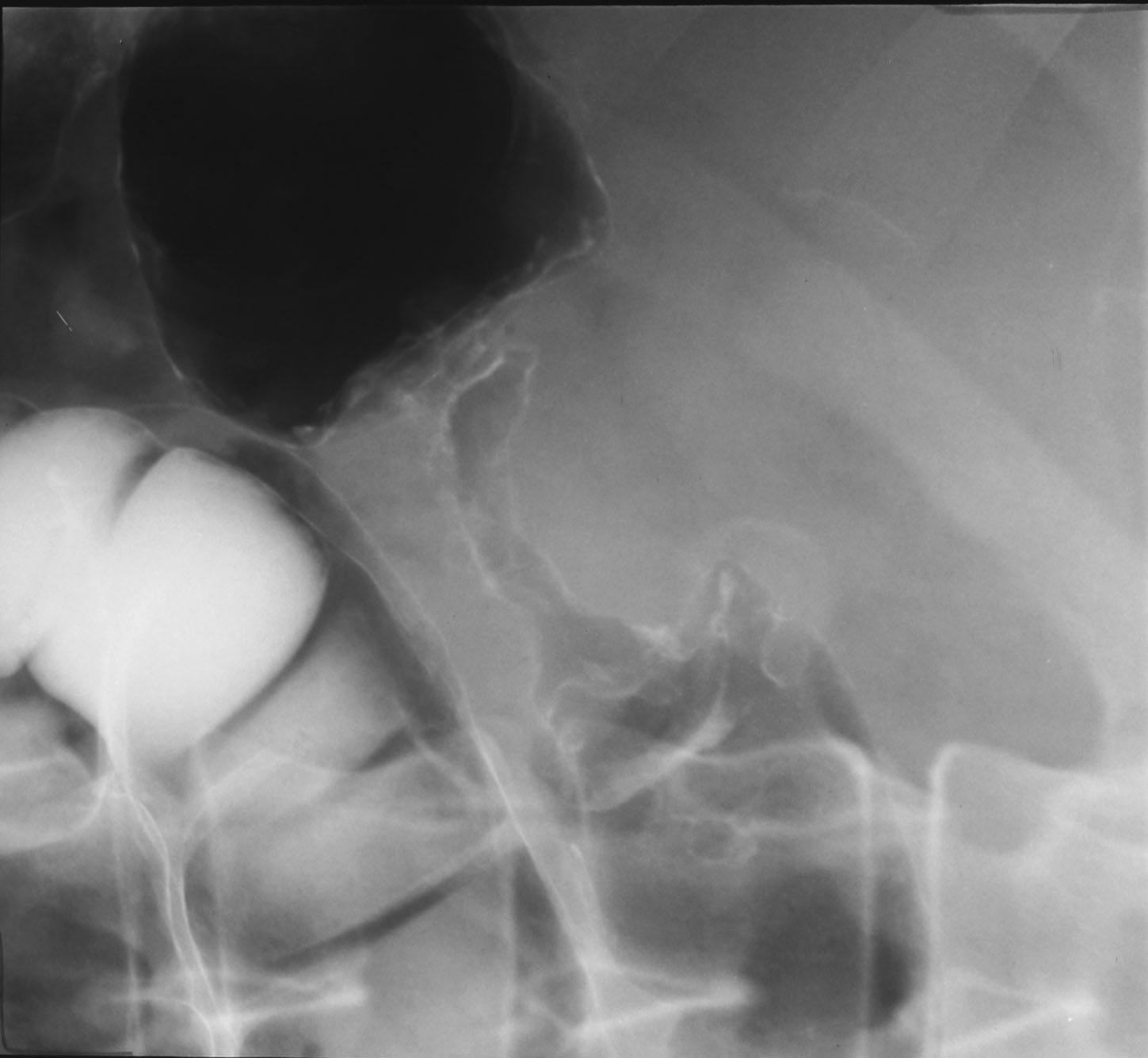
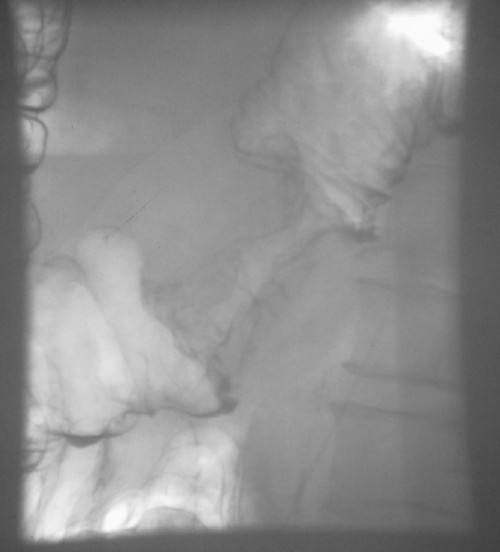
Oesophageal Obstruction (figure 16):

|
This shows complete oesophageal obstruction |
Small Bowel Obstruction (figures 21 & 22):

|
What are the characteristic features of small bowel obstruction on AXR?
- Dilated small bowel loops (greater than 3cm diameter)
- Central location of the small bowel
- Valvulae connivennte visible across bowel
- Multiple bowel loops (few in large bowel obstruction)
|